Varicose Veins
Which varicose vein treatment is best?
No single treatment is superior to the others. The best treatment for any individual will often depend on the size, location and number of damaged veins. You must also consider the success, potential risks and costs of treatment. Your physician will discuss these issues with you prior to starting any treatment.
It is very common for an individual to require a combination of treatment options to successfully treat their varicose veins. All treatments apart from conservative measures have risks. Please note that these risks are small and the overall results are generally excellent in the hands of knowledgeable and experienced physicians.
Everyone with venous insufficiency will benefit from lifestyle measures that include regular exercise,  maintaining a healthy weight, periodic rest and elevation of the legs, and wearing graduated compression stockings. All these measures help improve venous return.
maintaining a healthy weight, periodic rest and elevation of the legs, and wearing graduated compression stockings. All these measures help improve venous return.
 Exercise involving the legs will help the calf muscles pump more blood back towards the heart. Exercise also helps with maintaining a healthy weight.
Exercise involving the legs will help the calf muscles pump more blood back towards the heart. Exercise also helps with maintaining a healthy weight.
Weight loss reduces pressure on larger veins in the upper legs and abdomen and allows for easier return of venous blood.
Avoid prolonged periods of standing or sitting with legs dependant if possible and aim to rest and elevate the legs for 15 to 30 minutes three times a day. This reduces blood pooling in the leg due to gravity.
Finally the regular use of properly fitted graduated support stockings will help venous return when up on your feet for prolonged periods. These stockings provide the greatest compression around the foot and ankle and gradually reduce pressure as they move up the leg. Compression stockings will reduce pooling of blood in the superficial veins and the deep veins of the lower leg.
Medications such as horse chestnut extract can temporarily improve symptoms such as itching, aching or burning discomfort.
Lifestyle measures and medications can improve symptoms and help prevent further problems. However they cannot reverse existing damage and only further treatments (interventions) can remove spider or varicose veins. Learn more by contacting us today.
 very common cause of varicose veins. EVLT works by using laser energy to permanently collapse and seal shut damaged saphenous veins. This procedure is performed in a doctor's office or clinic under local anaesthetic only. A laser fibre is
very common cause of varicose veins. EVLT works by using laser energy to permanently collapse and seal shut damaged saphenous veins. This procedure is performed in a doctor's office or clinic under local anaesthetic only. A laser fibre is  inserted inside the damaged vein and is precisely positioned using ultrasound guidance. A freezing solution is delivered around the entire length of vein to be treated and then the laser fibre is pulled back sealing the vein as it is removed. The whole process takes less than one hour and you may be able to resume normal daily and work activities within 24 to 48 hours. In most cases no surgical incision is necessary. 98% of treatments are successful.
inserted inside the damaged vein and is precisely positioned using ultrasound guidance. A freezing solution is delivered around the entire length of vein to be treated and then the laser fibre is pulled back sealing the vein as it is removed. The whole process takes less than one hour and you may be able to resume normal daily and work activities within 24 to 48 hours. In most cases no surgical incision is necessary. 98% of treatments are successful.
Following EVLT you can expect to recover quickly with only minor discomfort. Post-procedure pain is much less than comparable surgery but you may experience a pulling or aching sensation in the treatment area for a few days. Bruising is common, but usually clears quite quickly (within 1 to 2 weeks).
EVLT treats the main superficial veins. Most of your visible varicose veins may be tributaries (or branches) of these main veins. Therefore following EVLT we allow 6 to 8 weeks for these branches to shrink and in many cases disappear completely. After 8 weeks any remaining branches may be treated with follow up sclerotherapy or ambulatory phlebectomy. The follow-up treatment is expected and is included as part of the EVLT treatment process.
Alternatives of EVLT - include surgical stripping or ligation (tying off the vein) alone. Advantages of EVLT- can be summarized as - early recovery and less pain, local anaesthetic only, few or no scars, high success rate, low complication rate.
 We may suggest sclerotherapy if you request or require treatment of small superficial varicose veins. This may be Conventional Sclerotheraphy by Oakville Vascular - Oakville, Ontario Canadayour only treatment or it may follow removal or ablation of larger varicose veins by alternative techniques.
We may suggest sclerotherapy if you request or require treatment of small superficial varicose veins. This may be Conventional Sclerotheraphy by Oakville Vascular - Oakville, Ontario Canadayour only treatment or it may follow removal or ablation of larger varicose veins by alternative techniques.
Sclerotherapy is performed in the office or clinic without the need for any anaesthetic. The sclerosing agent is injected directly into the vein using a very small needle. There a variety of sclerosants used but all act by causing inflammation and scarring to the inner wall of the vein. After the injection a compression bandage or stocking is applied to cause the vein walls to stick together and prevent blood from flowing into the damaged vein segment. This vein will then eventually scar, "dry up" and disappear.
Following sclerotherapy you can resume normal activities but must wear the compression bandage or stocking for 48 hours. Ideally you should be wearing compression stockings between treatments to prevent new veins from forming. There is a limit to the amount of sclerosing agent that should be given at any one time and typically people who have many clusters to be treated require multiple repeat visits. In addition many areas require repeat injections to get a good result.
Most treatments are successful but up to 10% of individuals may not respond to sclerotherapy - in some cases this is due to the fact the veins on the surface are being fed from deeper damaged veins that are not seen. Staining in the area of injection is common but is usually temporary (lasting 2 to 8 weeks), however some people may have permanent staining (2-5%).
Alternatives of conventional sclerotherapy - may include external laser (spider veins), or duplex-guided sclerotherapy or ambulatory phlebectomy (superficial branch veins).
Advantages of conventional sclerotherapy - little or no discomfort, no incisions, few complications (safe).
Disadvantages of conventional sclerotherapy - often need repeated sessions, may cause permanent staining, allergic reactions, skin ulcers in a small number of people.
 Ultrasound guided sclerotherapy uses agents identical to those used in conventional sclerotherapy but rather than injected as a liquid form, a foam may be used. Using ultrasound, the foam is injected into the veins that often lie hidden beneath the surface. Alternatively it may be used to inject larger superficial veins with more control. By using foam the sclerosing agent is less likely to be washed away in larger veins (as liquid would be) and will more likely cause the desired local damage to vein walls. As for conventional sclerotherapy, compression is applied after injection to cause the vein walls to stick together. By injecting the damaged larger or deeper veins, the smaller or more superficial visible veins will either disappear or respond better to conventional sclerotherapy. Ultrasound guided sclerotherapy has been used with considerable reported success in Europe, but is relatively new to North America. This technique requires more experience and skill than conventional sclerotherapy and does have the potential to cause staining, blood clots and allergic reactions. It does offer promise and will likely be a preferred treatment in the future for many people.
Ultrasound guided sclerotherapy uses agents identical to those used in conventional sclerotherapy but rather than injected as a liquid form, a foam may be used. Using ultrasound, the foam is injected into the veins that often lie hidden beneath the surface. Alternatively it may be used to inject larger superficial veins with more control. By using foam the sclerosing agent is less likely to be washed away in larger veins (as liquid would be) and will more likely cause the desired local damage to vein walls. As for conventional sclerotherapy, compression is applied after injection to cause the vein walls to stick together. By injecting the damaged larger or deeper veins, the smaller or more superficial visible veins will either disappear or respond better to conventional sclerotherapy. Ultrasound guided sclerotherapy has been used with considerable reported success in Europe, but is relatively new to North America. This technique requires more experience and skill than conventional sclerotherapy and does have the potential to cause staining, blood clots and allergic reactions. It does offer promise and will likely be a preferred treatment in the future for many people.
Following ultrasound guided sclerotherapy you should wear your compression bandage or stocking for 48 hours, but can resume regular activities immediately. Repeated sessions may be necessary to inject veins that remain open or to release trapped blood in damaged veins. Following successful treatment of the deeper veins, further treatment of superficial branches that may remain may be performed with techniques such as conventional sclerotherapy or ambulatory phlebectomy.
Alternatives to ultrasound guided sclerotherapy - is surgical ligation.
Advantages of ultrasound guided sclerotheraphy - no incisions, minimal pain and recovery time, enhances treatment of superficial veins.
Disadvantages of ultrasound guided sclerotheraphy - potential for blood clots, staining, long-term results unknown (relatively new treatment).
VenaSeal® Sapheon Closure System

VenaSeal® offers a minimally invasive treatment option that uses an advanced medical adhesive to seal the diseased vein.
The procedure is performed in a doctor’s office or clinic under local anesthetic only. A small catheter is inserted in the diseased vein and small amounts of adhesive are delivered through the catheter until the entire vein segment is sealed.
The entire procedure takes less than one hour.
After the procedure, a small bandage will be placed at the vein access site. Results vary, however most patients are able to return to normal activities immediately after the procedure.
Other Vascular Conditions
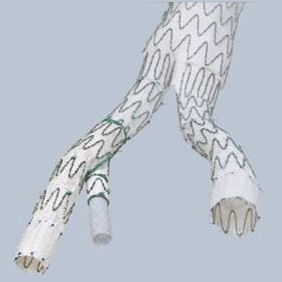
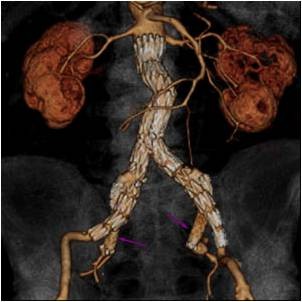
An abdominal aortic aneurysm (AAA) is a pathological increase in size of the main blood vessel in the abdomen. The normal aortic size is approximately 2 cm in men and a bit smaller in women. As the aorta increases in size, the risk of rupture increases. The condition is frequently silent and rupture can be the first symptom. Elective repair is available across Canada with significantly better outcomes when compared to those treated for aortic rupture. Abdominal aortic aneurysms (AAAs) are common and can be deadly if they are not treated. When aortic rupture occurs the majority do not survive.
Who is at Risk?
Five per cent of men and under one per cent of women over the age of 65 have an abdominal aortic aneurysm (AAA). All men between the ages of 65 and 75 and those under 65 with a family history should be screened. Women over 65 who are at high risk because of a smoking history and a family history should also be screened.
Screening
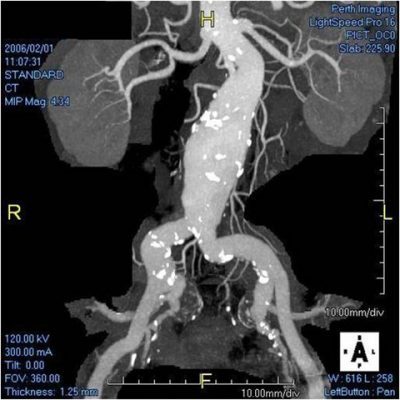
Abdominal aortic aneurysm screening uses ultrasound technology to measure the size of your abdominal aorta. The process is painless. You lie on your back on an exam table while a technologist applies gel to your abdomen. The technologist then takes images and measurements of your aorta by moving an instrument called a transducer across your abdomen.
This in-office screening procedure is available at Hamilton Vein Institute. Talk with your doctor today about abdominal aortic aneurysm screening.
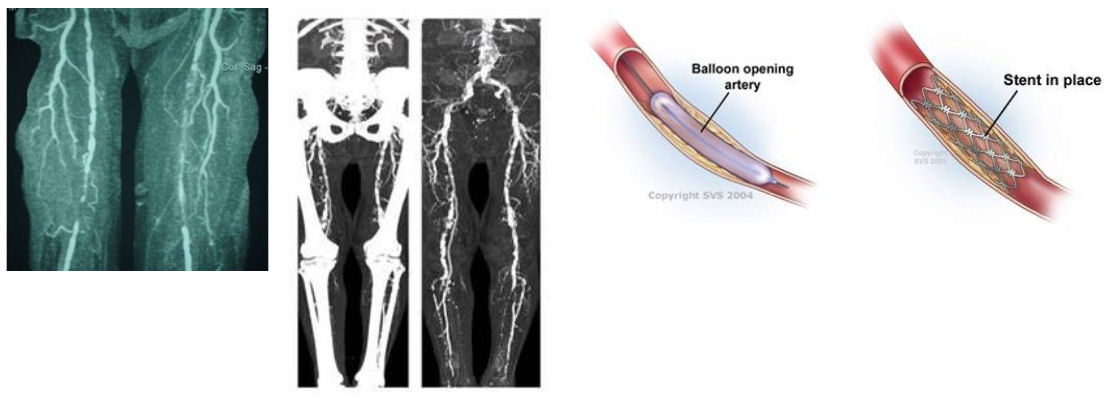
What is Peripheral Artery Disease (PAD)?
Normally the arteries carry blood away from the heart and deliver it to the body including the legs. This allows the leg muscles to exercise and work normally. PAD is a blockage in the circulation to the legs (poor circulation). This results in poor blood supply to the legs and feet which can result in leg pain or fatigue. In severe cases it can result in gangrene and amputation. PAD is a common cause of disability and is one of the more frequent manifestations of atherosclerosis or generalized vascular disease.
leg pain or fatigue. In severe cases it can result in gangrene and amputation. PAD is a common cause of disability and is one of the more frequent manifestations of atherosclerosis or generalized vascular disease.
What causes Peripheral Artery Disease?
PAD is caused by blockage in the arteries supplying blood to the legs. The cause of the blockage is atherosclerosis or "hardening" of the arteries. This is the same disease that can cause heart attacks and strokes but in this case it is affecting the arteries of the legs. Atherosclerosis occurs in the legs related to: smoking, diabetes, high blood pressure, elevated cholesterol, aging and heredity. Some of these factors can be controlled or treated, some can't.
What are the symptoms of Peripheral Artery Disease?
In it's mildest form PAD is silent, causes no symptoms and can only be detected with diagnostic testing. As PAD progresses patients develop pain or fatigue in the legs with exercise. This affects the major muscles of the calf , thigh or buttock. The discomfort usually occurs at the same distance of walking every time (consistent) and resolves within a few minutes of resting (relief). This is called claudication. When PAD is more severe there is pain even at rest and at night (usually in the foot). Skin breakdown (ulcer) or dead tissues (gangrene) can occur at this point. This is called critical limb ischemia. If this occurs there is a risk of amputation.
PAD Diagnosis and Testing
Usually a physical exam of the pulses of the leg and a simple Doppler ultrasound of the leg arteries will diagnose the presence and severity of PAD. Further testing with CT scan (a non invasive x-ray), MR scan (a non invasive magnetic scan) or an angiogram (an invasive x-ray) may be needed to plan the best treatment of PAD.
Lifestyle Modification for Peripheral Artery Disease
The most important thing for patients with PAD to do is to continue to exercise as much as they are able. Walking to the point of discomfort trains the leg muscles to work better and promotes improved circulation. It is also important to:
- stop smoking immediately
- loose weight if overweight
- diet to decrease cholesterol
- limit salt intake to decrease high blood pressure
Treatment for Peripheral Artery Disease
Our team of vascular specialists will provide you with the best treatment options based on your diagnosis.
What is Carotid Artery Disease?
The carotid arteries are the two large vessels that run up either side of the neck. They then divide into two large branches. One is the external carotid artery that supplies blood to the face and neck. The other is the internal carotid artery and it supplies blood to the eye and brain. The point at which the artery divides is slightly wider and is called the carotid bulb. Atherosclerosis, or plaque formation, seems to occur preferentially at this site, causing narrowing of the blood vessel and reduces blood flow to the brain and eye. This can result in stroke or blindness.
What causes Carotid Artery Disease?
A build up of plaque made up of cholesterol, calcium, fibrotic tissue and cellular debris called atherosclerosis thickens and narrows the arteries in the neck. Sometimes this plaque softens and breaks open. When this happens, clot-forming cells called platelets stick to the plaque. Sometimes the whole artery will clot and reduce the flow of blood to your brain causing a stroke. More often, debris from the plaque or bits of platelet plug will travel up the artery, blocking the blood vessels within the eye or brain, causing blindness or stroke.
What are the symptoms of Carotid Artery Disease?
Carotid artery disease occurs more frequently as we age and affects up to 3% of the general population. Most of the time there are no symptoms. The first symptom may be a stroke with tingling or weakness of one side of the body or face, slurred speech or difficulty speaking or sudden blindness in one eye. Sometimes these symptoms only last a short time and resolve totally. This is a mini-stroke or TIA (transient ischemic attack). Just because the symptoms go away, it is still important to seek medical attention immediately. These mini-strokes can be an early warning of impending major, permanent stroke if they are not investigated and treated.
When should I see my doctor?
If you experience sudden weakness or tingling of one of your arms, legs, or one side of your face, slurred speech or difficulty speaking or blindness in one eye, you should seek medical attention immediately, even if the symptoms completely resolve after a short time. If you smoke, have high blood pressure, diabetes, high cholesterol and/or a family history of atherosclerosis, you should see your doctor regularly for counselling and treatment of these conditions to reduce your likelihood of developing carotid artery disease.
Diagnosis and tests for Carotid Artery Disease
Your doctor will start by taking a health history and examining you. This will help determine your risk factors for developing carotid artery disease. These include smoking, high blood pressure, high cholesterol and family history. The first test your doctor will usually order is an ultrasound of the carotid vessels. This is a non-invasive test that uses sound waves to look at the carotid arteries and to assess the blood flow through them. Sometimes more information is required and a CT angiogram or Magnetic Resonance Angiogram (MRA) may be ordered. These tests involve giving contrast (dye) and use of either x-rays for CT, or magnetic fields for MRA to create a picture of the artery.
Lifestyle modification for Carotid Artery Disease
If you smoke you are very likely to develop progressive atherosclerosis. Quitting smoking will not necessarily reverse the formation of plaque in the carotid arteries but it may stop the progression of narrowing and reduce the possibility of plaque breakdown that can trigger a stroke. Other factors such as exercise, weight loss and a diet low in saturated fat can reduce the risk of developing atherosclerotic disease.
Non-surgical and Medical Management for Carotid Artery Disease
Medications that prevent platelets from sticking to the plaque surface are important in preventing stroke. The most commonly used medication for this is aspirin. A dose of 81 - 325 mg daily is recommended. If you are intolerant of aspirin, your doctor will discuss alternate medications that can be used. Studies have also shown that being on a statin agent for cholesterol control can induce remodelling and even regression of the carotid plaque. High blood pressure itself is a risk factor for stroke and developing atherosclerosis and should be treated with medication. If you are diabetic, good control of your blood sugar levels is also important.
Guidelines for Intervention for Carotid Artery Disease
The goal of intervention on a carotid narrowing is to reduce your risk of stroke. If you have had a non-disabling stroke or TIA due to carotid stenosis and have over 70% narrowing, your doctor will usually recommend intervention to get rid of the narrowed area, either with surgery or angioplasty, described below. If you have symptoms and 50-69% narrowing, intervention may be recommended, but risk factor treatment and medication changes might be tried first. If you have no symptoms of stroke or TIA, the recommendation for intervention is often based on factors such as your age, degree of narrowing and medical fitness for the procedure.
Treatment for Carotid Artery Disease
There are several treatment options available for carotid artery disease ranging from endovascular treatments including angioplasty and stenting, to surgical procedures. Our team at Hamilton Vein Institute will provide you with the treatment options based on your diagnosis.